Physical Therapist's Guide to Cubital Tunnel Syndrome
Cubital tunnel syndrome is the second most common nerve compression occurring in the arm. (Carpal tunnel syndrome is the most common.) It is a condition caused by increased pressure on the ulnar nerve at the elbow. This pressure can result in discomfort and pain, and may progress to loss of function of the hand. Cubital tunnel syndrome generally affects men more than women, especially those with jobs that require repetitive elbow movements and a bent elbow position, such as using tools like drills at work, talking on the phone, doing computer work, painting, or playing an instrument. Physical therapists help people with cubital tunnel syndrome reduce pain and swelling and restore normal movement and function to the arm, wrist, and hand.
What is Cubital Tunnel Syndrome?
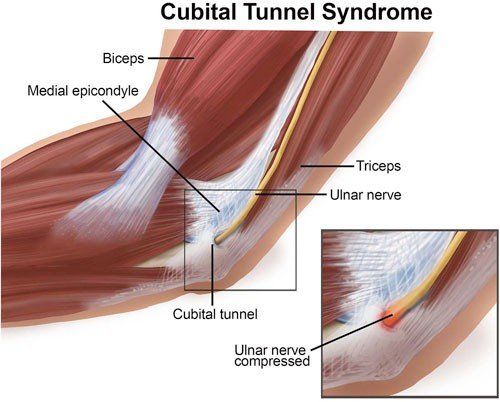
Cubital tunnel syndrome is caused by compression of the ulnar nerve when it passes under a bony bump (the medial epicondyle) on the inside portion of the elbow. In this area, the nerve is relatively unprotected and can be trapped between the bone and the skin in a tunnel called the cubital tunnel. Although it is not an actual bone, this area is commonly called your “funny bone.” When you hit the funny bone just the right way, you have actually hit the ulnar nerve. This contact sends a sensation of tingling, numbness, burning and/or pain along the inside of your arm and down to the ring and little fingers. When the ulnar nerve is compressed, it causes the same type of symptoms. The ulnar nerve can be pinched at any point along its length, but the most common site of compression is on the cubital tunnel.
Cubital tunnel syndrome often results from prolonged stretching of or pressure on the ulnar nerve. When the arm is bent for a long time, such as when holding the phone, it stretches the ulnar nerve across the inside of the elbow, creating a traction force that decreases the blood flow to the nerve and may cause nerve irritation. Prolonged pressure on the nerve may happen, for example, when the elbow and lower arm lean against a table and the ulnar nerve is pushed over the bone, which may cause the sensation of tingling, numbness, burning and/or pain along the inside of your arm and hand.
Signs and Symptoms
Cubital tunnel syndrome can occur after a traumatic incident, such as an elbow fracture, or develop slowly over time. It usually begins with numbness and/or tingling, or burning on the inside of the forearm extending down into the hand. Typical symptoms include:
- Intermittent pain, numbness, and tingling brought on by sustained bending of the elbow
- Tenderness on the inside of the elbow where the nerve is close to the surface
Later symptoms sometimes include:
- Difficulty gripping and holding on to objects
- Muscle wasting of the small muscles of the hand
- A hand deformity in which the small and ring fingers bend inward, referred to as an "ulnar claw hand"
CAUTION: More severe symptoms, especially those with muscle wasting and hand deformities, should be evaluated by a physician.
How Is It Diagnosed?
Cubital tunnel syndrome can be diagnosed by a physical therapist or a physician. Your physical therapist will typically perform a comprehensive evaluation that should include assessment of your neck to rule out compression of the nerve where it starts in the neck. To confirm the compression of the ulnar nerve is occurring at the elbow, your physical therapist may use the following tests and examination:
- Observation and inspection of the elbow and forearm
- Touching and moving the arm in the area of the nerve to determine its relationship to the elbow and its stability in the groove behind the elbow where the nerve travels
- Tapping the nerve at the elbow (the Tinel's sign test)
- Assessing the flexibility of the ulnar nerve
- A sensory examination that includes both light touch, a test of the ability to distinguish between sharp or dull stimulus, and the ability to distinguish 1 point from 2 points (2-point discrimination)
- Checking the strength of specific muscles of your hand
- Checking your pinching and gripping ability
Cubital tunnel syndrome can be accurately diagnosed clinically without additional testing. Occasionally you may be referred for electrodiagnostic tests called electromyography (EMG) and/or a nerve conduction study (NCS). These tests evaluate the ability of the nerve to conduct signals along its full length. They can help determine the exact site of the compression and estimate the extent of the compression.
If your physical therapist considers your symptoms to be more severe, the therapist may refer you to a physician for an additional assessment.
How Can a Physical Therapist Help?
Many cases of mild to moderate cubital tunnel syndrome can be treated without surgery. Your physical therapist will determine the activities that bring on your symptoms. The recommendations at this point will be to avoid those activities for a time. Remember, the nerve is irritated and at times swollen. If the irritation and swelling can be reduced, the symptoms should resolve.
In more advanced cases, your physical therapist will modify your activity and may recommend you use a splint to take the pressure off the nerve. As your condition begins to improve, your physical therapist may teach you:
Range-of-motion exercises. Your physical therapist will show you specific exercises to help return full length to the muscles of the arm that have shortened due to protective posturing, and to maintain the normal length of those that have remained unaffected.
Muscle strengthening exercises. Improving strength in the surrounding muscles can help reduce pain and improve functional ability.
Nerve gliding exercises. Nerves have the ability to be stretched, just like muscles or joints. Nerve tissue is the strongest, longest tissue in the body and the one most sensitive to stretching. In cubital tunnel syndrome, the nerve can become tight or trapped; these exercises are an effective means of promoting blood flow to the ulnar nerve and gently stretching it.
Ergonomic training. Your physical therapist will teach you ways to avoid positions and postures that compress or put prolonged stretch on the ulnar nerve. You may need to learn how to modify work and self-care activities to prevent further nerve irritation.
If Surgery Is Required
More severe or prolonged cases of cubical tunnel syndrome may require surgery. The longer you have experienced symptoms and the more you experience weakness, numbness, tingling, and pain the more likely you are to need surgery. The goal of surgery is to relieve the pressure on the ulnar nerve.
Your physical therapist will design an individual program of postsurgical physical therapy based on the nature of your operation and the surgeon’s instructions. Each surgery will require a unique treatment regimen, but your postsurgical rehabilitation will involve many of the elements discussed above. Activity modification will be a big part of your postsurgical rehabilitation to prevent recurrence of your symptoms.
Can this Injury or Condition be Prevented?
Little is known about prevention of cubital tunnel syndrome. Often, the syndrome is not diagnosed until symptoms are already present. However, some general precautions may be taken.
- Obesity has been linked by some researchers to cubital tunnel syndrome. Healthy lifestyle choices and a reduction in your weight may help prevent its development.
- People in occupations that require holding the elbow in a bent position, such as computer programmers, should be encouraged to perform consistent positional changes to take stress off the ulnar nerve.
- Diabetes has been recognized as a risk factor.
- Knowledge of how to avoid positions and activities that can cause ulnar nerve irritation may help prevent injury. Modifications to daily activities such as avoiding positioning the elbow in a bent position for a prolonged period of time, and not resting the elbow on hard surfaces can help. At work, finding ways to limit repetitive motions and the use of vibratory tools (such as drills) may decrease risk.
Your physical therapist will teach you movement and lifestyle modifications to help prevent recurrence of cubital tunnel syndrome once it has been diagnosed.
MoveForwardPT.com, the official consumer Website of the American Physical Therapy Association,© 2017